Squint is the term used when the eyes are not exactly straight. When looking at an object, normal eyes will look exactly in the same direction. This is required for the light to fall on exactly the same parts of the two retinas(the backs of the eyes). If a squint is present the two eyes cannot focus on exactly the same point.
Types
The severity can vary. Some squints are very marked and obvious. Some only become noticeable when the child is tired. Some are quite small and are only discovered by a proper examination.
The cause can vary. Sometimes they are due to muscle or nerve problems of the eye. Sometimes eye diseases cause a squint. However, the majority are due to one eye being more longsighted than the other. In this common situation one eye has to strain more than the other to see clearly and this can lead to a squint.
The direction can vary. Most are convergent i.e. the squinting eye tends to look inwards. However, the squinting eye can be divergent(looking outward) or looking up or down.
Broadly Squint is divided in 2 types:
- Incommitant(where the degree of squint varies in different directions)
- Commitent(where the squint in all directions of gaze remains the same)
The Incommitent squint is mainly due to paralysis of one or muscles of the eye.
The Commitent type has multiple reasons. It is broadly classified as
- Exotropia(eyes move out)
- Esotropia(Eyes move inwards)
- Vertical squints(misalignment of eyes in vertical direction)

Exotropia
Exotropia is the outward deviation(turn) of an eye. The deviation may occur while fixating(looking at) distant objects, near objects or both. Fortunately, most exotropia is intermittent and this means that the eye deviation or turn occurs only some of the time. As long as the eyes are straight some of the time, the brain will develop some normal functioning of the eyes(stereoscopic depth perception). Since the brain and eyes work properly some of the time, time is on your side.
Treatment for intermittent exotropia does not have to occur immediately. As a matter of fact, early surgery has the potential of disturbing the ability of the brain for fusion in the future and can cause a permanent reduction in vision (Amblyopia).
When the turn occurs during distance viewing the major problem is cosmetic. The child might be accused of daydreaming or not paying attention. The parents will often notice the turn and then they bring their child to the eye doctor who might not find it. This is because the turn usually occurs during times of inattention, fatigue, or distance viewing not during the anxiety-provoking eye examination. These children often close their eye in bright sunlight.
If the squint is constant and is causing disruption of the ability of stereopsis(three dimensional vision) then corrective muscle surgery is the only tretment.
 Esotropia
Esotropia
Esotropia can be divided into various categories each requiring a different treatment plan, each having a different prognosis.
Types of Esotropia
There are following 4 types of Esotropia:
- Congenital Esotropia
- Infantile Esotropia
- Accommodative Esotropia
- Partially Accommodative Esotropia

Congenital and Infantile Esotropia
Congenital means from birth and, using this strict definition, most infants are born with eyes that are not aligned at birth. Only 23% of infants are born with straight eyes. In the majority of cases, one eye or the other actually turns outward during the neonatal period. Within the first three months the eyes gradually come into more consistent alignment as coordination of the two eyes together as a team develops.
It is common for infants to appear as if they have Esotropia, or inward turn of the eyes, because the bridge of the nose is not fully developed. This false or simulated appearance of an inward turning is known as Epicanthus. As the infant grows, and the bridge narrows so that more of the white of the eyes(Sclera) is visible on the inner side, the eyes will appear more normal.
True Congenital Esotropia is an inward turn of a large amount, and is present in very few children, but the infant will not grow out of this turn. True Infantile Esotropia usually appears between the ages of 2 and 4 months.
The baby with Infantile Esotropia usually cross fixates, which means that he or she uses either eye to look in the opposite direction. The right eye is used to look toward the left side, and the left eye is used to look toward the right side. By definition, they alternate which eye they are looking with. It is more difficult to help this type of Strabismus with non-surgical methods, such as vision therapy and/or glasses. Sometimes, clear tape applied to the inner third of each lens(Occlusion) can reduce the tendency to turn inward. Prisms may aid alignment if the turn is not too large.
Some children who develop Strabismus, in which coordination between the two eyes is poor, also have a typical gross motor development patterns. They typically skip the crawling stage with bilateral movements, and go right from creeping to standing. The interplay between gross motor, particularly balance systems(Cerebellar and Vestibular) and Binocular Systems(motor control of the two eyes) is evident in the large number of young children with Cerebral Palsy who have Strabismus.
If the inward turn of the eye is constant, and of a large amount, surgery may be indicated. Both the parent and surgeon have to be committed to multiple procedures to obtain perfect alignment. Improved alignment may look better cosmetically, but it does not necessarily enable the brain to utilize information from both eyes together. Stereopsis, or two-eyed depth perception, is often poor following surgical treatment. The best chance for visual success occurs when the surgeon works with an Optometrist who is comfortable in prescribing glasses and exercises to encourage perfect alignment of the eyes with proper fusion. This model of cooperative care is similar to the relationship between the orthopedic surgeon and physical therapist.
If Amblyopia is present(poorer vision in the turned eye), therapy including patching is often required so that the turned eye develops the capacity to see as well as the better eye. It is best to do this before surgery.
The chance of developing Binocular Vision with surgery alone diminishes with age. Older children with Infantile Esotropia may need both surgical intervention and vision therapy. Smaller turns may only require vision therapy. Getting the eyes to work together requires a lot of time and effort, but is usually worth it.
Accomodative Esotropia
 If excessive inward turning of an eye is first noted around 2 years of age, it may be due to difficulty integrating the focusing(accommodative) system with the eye alignment(binocular) system. Normally when we look across the room or beyond, our eyes are parallel, or straight. However, when we look at things up close, two things happen. We need to converge more(aim both eyes inward at the same time) and we have to input more focus, or accommodate to keep things clear. Children have large amounts of focusing power, and sometimes in getting things clear, inward turning or Esotropia results. If the inward turning only occurs up close, as when playing with small objects, making eye contact, coloring, looking at picture books and so forth, the child may just need glasses for near activities to reduce or eliminate the esotropia.
If excessive inward turning of an eye is first noted around 2 years of age, it may be due to difficulty integrating the focusing(accommodative) system with the eye alignment(binocular) system. Normally when we look across the room or beyond, our eyes are parallel, or straight. However, when we look at things up close, two things happen. We need to converge more(aim both eyes inward at the same time) and we have to input more focus, or accommodate to keep things clear. Children have large amounts of focusing power, and sometimes in getting things clear, inward turning or Esotropia results. If the inward turning only occurs up close, as when playing with small objects, making eye contact, coloring, looking at picture books and so forth, the child may just need glasses for near activities to reduce or eliminate the esotropia.
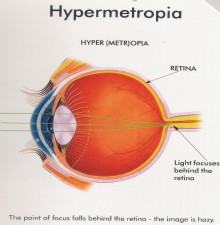
 However, if a child is significantly farsighted(Hyperopia), an inward turn of the eye may even occur when focusing to look further away, such as television. If the amount of turn is greater at near than far, your optometrist may prescribe a multifocal lens. For children this could be a traditional bifocal with a line, or a form of no-line bifocal or progressive lens. Your optometrist will review with you which is the best option for your child. In addition, vision therapy may be of benefit. This condition should never be treated with surgery.
However, if a child is significantly farsighted(Hyperopia), an inward turn of the eye may even occur when focusing to look further away, such as television. If the amount of turn is greater at near than far, your optometrist may prescribe a multifocal lens. For children this could be a traditional bifocal with a line, or a form of no-line bifocal or progressive lens. Your optometrist will review with you which is the best option for your child. In addition, vision therapy may be of benefit. This condition should never be treated with surgery.
When the eyes are aligned by corrective lenses sometimes the eyes spontaneously begin to work together. Other times, they need help. Remember, the habit of suppressing or turning off one eye or the other was probably developed over a number of years. The eyes have to be trained to work together again and suppression must be eliminated in order to restore normal eye teaming, depth perception, and stereopsis. The eye doctor might have to patch an eye that was suppressed or turned off and/or employ vision therapy.
Intermittent turns usually do not require long term treatment. Vision Therapy may be necessary to improve the muscle coordination and eventually eliminate the bifocal.
Patients with Accommodative Esotropia should never have eye muscle surgery to eliminate the need for glasses. If they do, they will have significant focusing problems when they get older. In the future, these patients might be excellent candidates for refractive surgery(Hyperopic LASIX) or contact lenses. This should be coordinated with the developmental Optometrist and LASIK surgeon.
Partially Accommodative Esotropia
In some instances, part of the inward turn is due to basic Esotropia, and an additional amount due to the effect of accommodation. Glasses may reduce the amount of eye turn, but it is not totally compensated. Initially, the eye doctor may prescribe prism to compensate for the amount of turn. Office-based Vision Therapy is usually needed. Surgery remains an option to address the non-accommodative portion of the Esotropia. Remember that surgery alone rarely enables a patient to learn how to use both eyes together as a team, and usually leaves the patient with poor Stereopsis. Because vision is a learned process, some form of therapy is often helpful in learning new binocular vision patterns, or restoring normal pathways that have been lost or underutilized. Binocular vision occurs in the visual centers of the brain, not in the eye muscles.
Hypertropia
 Upward deviation of the eye is usually due to a paresis of one of the muscles that either elevate or depress the eye. Most of the time it is due to one specific muscle known as the Superior Oblique. The paresis may be congenital(born with it) or acquired. Most of the time, palsy of the superior oblique is congenital but may present itself later in life. For one reason or another the fusion system breaks down and the deviation becomes manifest. An inexperienced doctor may send this patient out for extensive neurological testing including MRI. There are tell tale signs that tell the sophisticated doctor that the turn has been there a long time and one does not have to worry about it such as a head tilt being present in old pictures, etc.
Upward deviation of the eye is usually due to a paresis of one of the muscles that either elevate or depress the eye. Most of the time it is due to one specific muscle known as the Superior Oblique. The paresis may be congenital(born with it) or acquired. Most of the time, palsy of the superior oblique is congenital but may present itself later in life. For one reason or another the fusion system breaks down and the deviation becomes manifest. An inexperienced doctor may send this patient out for extensive neurological testing including MRI. There are tell tale signs that tell the sophisticated doctor that the turn has been there a long time and one does not have to worry about it such as a head tilt being present in old pictures, etc.
If the Hypertropia is a decompensation of a congenital deviation, then treatment may consist of prism glasses and vision therapy. Our goal is fusion without prismatic glasses. However, often, treatment requires small amount of prism to hold the eyes in comfortable alignment.







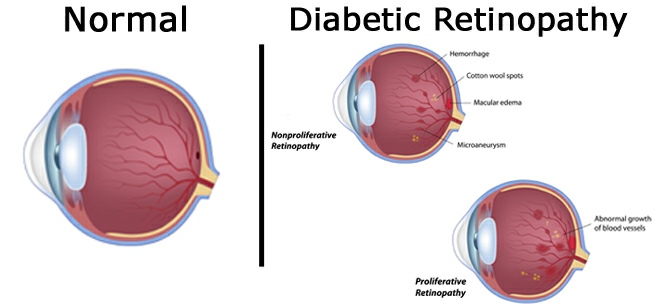



 Your eye care professional may suggest laser surgery in which a strong light beam is aimed onto the retina. Laser surgery and appropriate follow-up care can reduce the risk of blindness by 90 percent. However, laser surgery often cannot restore vision that has already been lost. That is why finding diabetic retinopathy early is the best way to prevent vision loss.
Your eye care professional may suggest laser surgery in which a strong light beam is aimed onto the retina. Laser surgery and appropriate follow-up care can reduce the risk of blindness by 90 percent. However, laser surgery often cannot restore vision that has already been lost. That is why finding diabetic retinopathy early is the best way to prevent vision loss. The study found that the group that tried to keep their blood sugar levels as close to normal as possible also had much less kidney and nerve disease. This level of blood sugar control may not be best for everyone, including some elderly patients, children under 13, or people with heart disease. So ask your doctor if this program is right for you.
The study found that the group that tried to keep their blood sugar levels as close to normal as possible also had much less kidney and nerve disease. This level of blood sugar control may not be best for everyone, including some elderly patients, children under 13, or people with heart disease. So ask your doctor if this program is right for you.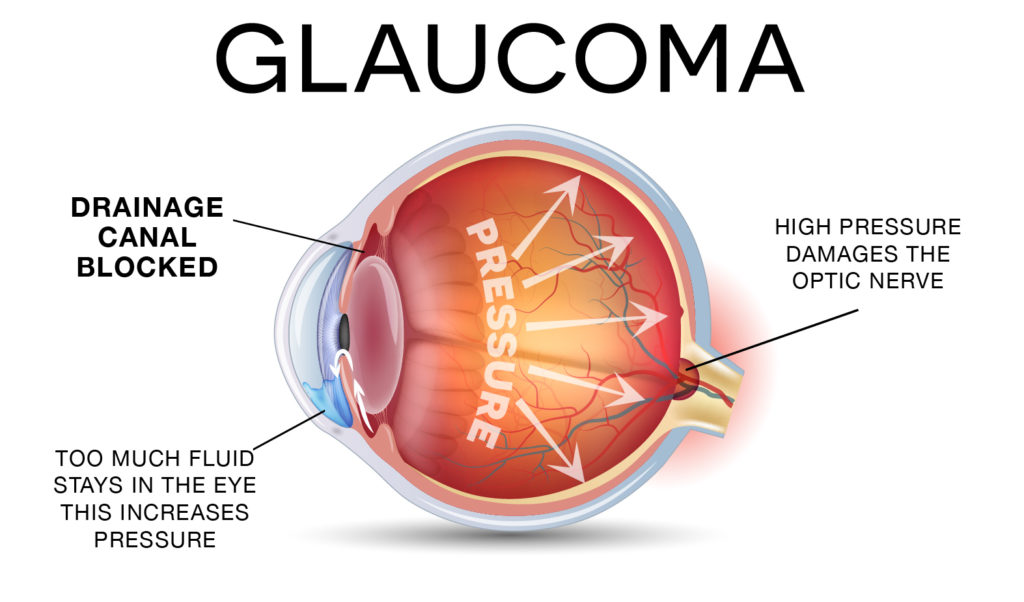
 Staining of the Cornea and Conjunctiva with special dye like Fluoroscein and Rose Bengal are some of the other ways to diagnose dry eye.
Staining of the Cornea and Conjunctiva with special dye like Fluoroscein and Rose Bengal are some of the other ways to diagnose dry eye.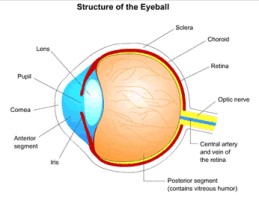


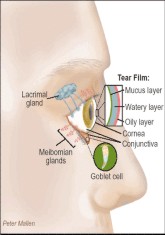
 Tear apparatus of the eye: Tears are formed in the Lacrimal Glands and the Accessory Lacrimal Glands. They are drained via the Lacrimal Ducts, at the nasal side of the eye, into the Nasolacrimal duct, which opens into the nose. That is why any eyedrops applied to the eye come into the nose and throat. Sometimes the Nasolacrimal duct may get blocked and it may then need to be openned surgically.
Tear apparatus of the eye: Tears are formed in the Lacrimal Glands and the Accessory Lacrimal Glands. They are drained via the Lacrimal Ducts, at the nasal side of the eye, into the Nasolacrimal duct, which opens into the nose. That is why any eyedrops applied to the eye come into the nose and throat. Sometimes the Nasolacrimal duct may get blocked and it may then need to be openned surgically. Cross-section of the eyelid: The tarsal plate is like a backbone of the eyelid. It gives strength and flexibility to the eye lid. The muscles in the lid are attached to this structure. The Meibomian Glands are like sweat glands. It secretes a fatty substance which helps in maintaining the surface tension of the tears. A blockage of these glands leads to a condition called Chalazion.
Cross-section of the eyelid: The tarsal plate is like a backbone of the eyelid. It gives strength and flexibility to the eye lid. The muscles in the lid are attached to this structure. The Meibomian Glands are like sweat glands. It secretes a fatty substance which helps in maintaining the surface tension of the tears. A blockage of these glands leads to a condition called Chalazion. Cross-section of the Cornea: Cornea is the front transparent layer of the eye. It is a multi layered structure. The tears also form a thin layer on top of the cornea and protect and nourish it. A deficiency of tears can cause Dry eye. Shape of the Cornea is altered with LASER in Refractive Surgery(Surgery for correcting spectacle numbers). Any opacity or injury to this structure can cause permanent opacity and hence loss of vision.
Cross-section of the Cornea: Cornea is the front transparent layer of the eye. It is a multi layered structure. The tears also form a thin layer on top of the cornea and protect and nourish it. A deficiency of tears can cause Dry eye. Shape of the Cornea is altered with LASER in Refractive Surgery(Surgery for correcting spectacle numbers). Any opacity or injury to this structure can cause permanent opacity and hence loss of vision. Division of the eye: The eye is divided in two main parts. The front or Anterior Segment. This has a water like fluid called Aqueous Humor.The back part or Posterior Segment has a thick jelly like substance called Vitreous Humor.
Division of the eye: The eye is divided in two main parts. The front or Anterior Segment. This has a water like fluid called Aqueous Humor.The back part or Posterior Segment has a thick jelly like substance called Vitreous Humor. Anterior Segment of the eye: It also has 2 sub-sections divided by the Iris. The Iris is like the shutter of camera. It controls the amount of light coming in the eye. The Aqueous Humor enters the chamber from the Ciliary Body and passes through the hole in the Iris called the Pupil, to exit in the angle between the Iris and Cornea. Any obstruction in the circulation of this fluid leads to rise in the eye pressure and can then cause a condition called Glaucoma.
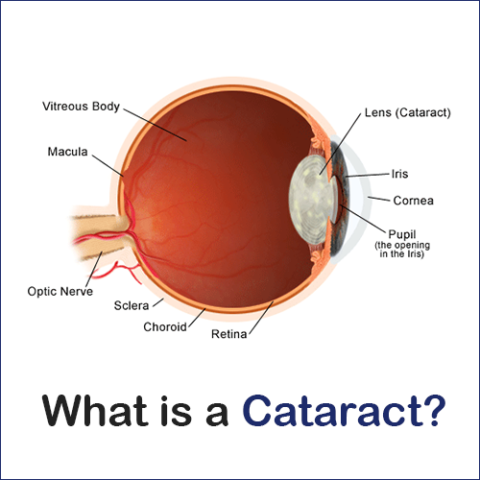
Anterior Segment of the eye: It also has 2 sub-sections divided by the Iris. The Iris is like the shutter of camera. It controls the amount of light coming in the eye. The Aqueous Humor enters the chamber from the Ciliary Body and passes through the hole in the Iris called the Pupil, to exit in the angle between the Iris and Cornea. Any obstruction in the circulation of this fluid leads to rise in the eye pressure and can then cause a condition called Glaucoma. Lens of the eye: When this becomes opaque, it is called Cataract. Surgery is the only treatment for Cataract.
Lens of the eye: When this becomes opaque, it is called Cataract. Surgery is the only treatment for Cataract. Front view of the Retina: Retina is inner layer of the eye which when stimulated by light sends signal to brain and we perceive an image. The retina may get detached from the inner layer and is then put in its place by surgery. Diseases like Diabetes, High Blood pressure, old age, high myopia, etc can also damage the retina and can cause permanent loss of vision.
Front view of the Retina: Retina is inner layer of the eye which when stimulated by light sends signal to brain and we perceive an image. The retina may get detached from the inner layer and is then put in its place by surgery. Diseases like Diabetes, High Blood pressure, old age, high myopia, etc can also damage the retina and can cause permanent loss of vision. Cross-section of the Retina: Retina is made up of 10 layers. Signal from here are carried by the Optic Nerve to the brain via the visual pathway. The Optic Nerve can be affected in many disease, like Glaucoma and Alcohol abuse.
Cross-section of the Retina: Retina is made up of 10 layers. Signal from here are carried by the Optic Nerve to the brain via the visual pathway. The Optic Nerve can be affected in many disease, like Glaucoma and Alcohol abuse. Eye Muscles: They control the eye movement. Any imbalance in the tone of these muscles can lead to Squint. Sometimes surgery is necessary to restore the proper balance.
Eye Muscles: They control the eye movement. Any imbalance in the tone of these muscles can lead to Squint. Sometimes surgery is necessary to restore the proper balance.